This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box.
A 53 year old male patient, resident of Pochampally, agricultural worker (toddy tree climber) by occupation came to the OPD with chief complaints of:
Chief Complaints:
Difficulty in passing urine since 10 days
Leg swelling since 5 days
Breathlessness since 4 days
History of Presenting Illness:
Patient was apparently asymptomatic 10 days back, then he developed difficulty in passing urine, associated with pricking type of pain, non blood tinged, clear in appearance.
He also developed irregular passing of stools of frequency once in 2 days after using medication.
Then he developed bilateral swelling of both lower limbs, sudden in onset and gradually progressive not associated with pain.
Later he also developed dyspnoea, insidious in onset and gradually progressive - Grade 4 (occurred even during rest) aggravated during rest and relieved on walking. (Orthopnea+)
Patient also has cough which is productive, non blood tinged, non foul smelling.
No history of palpitations/ burning micturition
Past History:
Known case of Hypertension (using medication)
Known case of Diabetes (initially used medication then stopped)
N/K/C/O Epilepsy, Thyroid.
Personal History:
Diet Mixed
Decreased Appetite
Decreased Urine Output
Decreased Bowel Moments
Consumes Alcohol - Occasionally (2 times per week)
Consumes Cigarettes- Pack per week
Family History:
No similar complaints in the family.
General Examination:
Vitals:
BP: 160/80 mmhg
RR: 19 cpm
HR: 68 bpm
Pallor: Present
Icterus: Absent
Cyanosis: Absent
Koilonychia: Absent
Lymphadenopathy: Absent
Edema: Bilateral Pedal Edema
Systemic Examination:
Patient is conscious, coherent, co-operative
CVS:
S1, S2 heard
Respiratory Rate:
Trachea Position Central
Biphasic Stridor present
Laboured Respiration present
CNS:
No neurological deficits present
Abdomen:
Umbilicus everted and central
No scars found
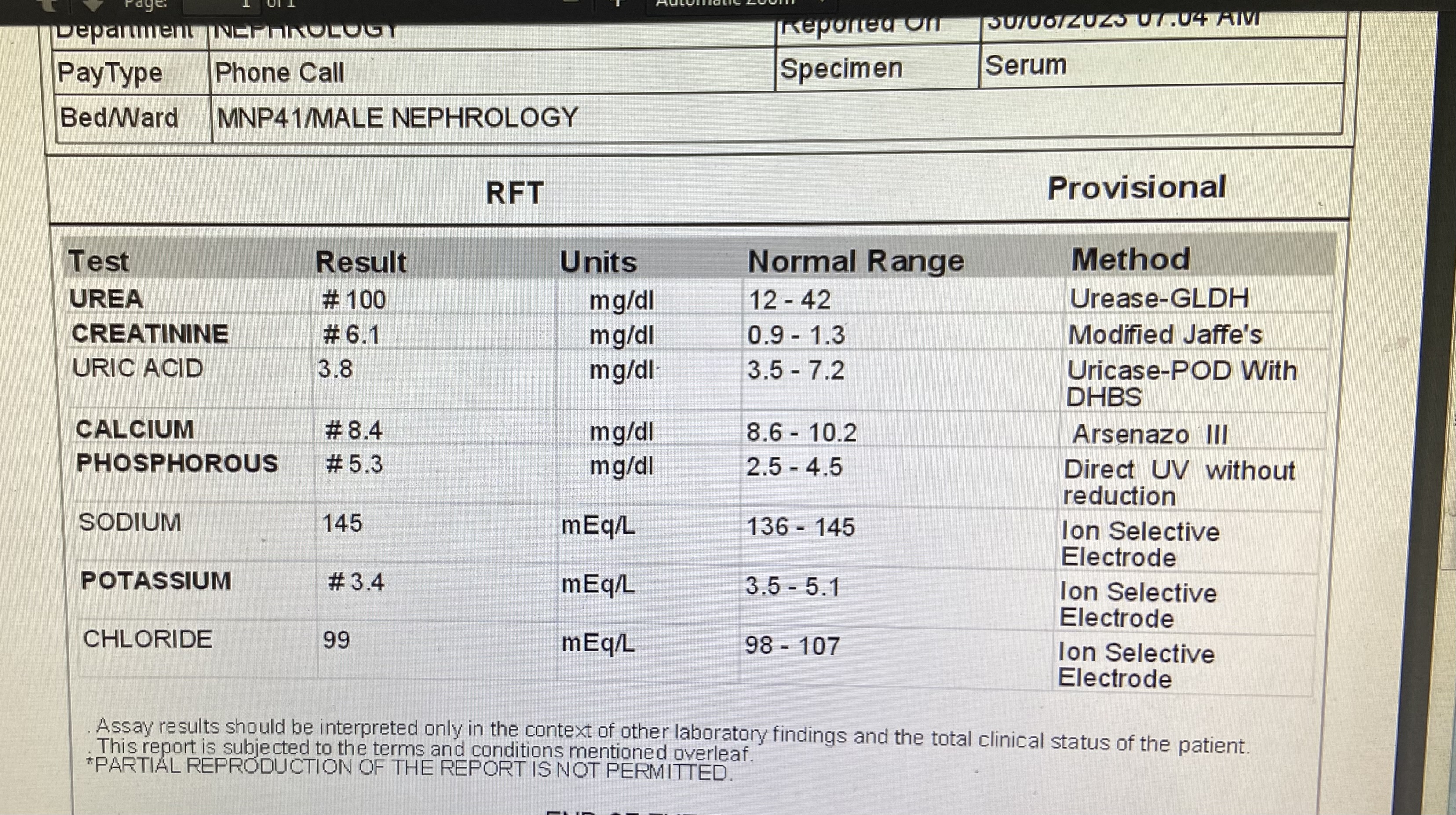
Provisional Diagnosis:
Chronic Kidney Disease
Treatment History:
2-9-23
Inj. Lasix - 40 mg
Inj. Piptaz - 2.25 gm
Tab. Nifidipine - 20 mg
Tab. Clonidine - 0.1 mg
Tab. Orofer - 1 Tab
Tab. Shelcal - 500 mg
Nab. Budecort
CBP -30-8-23

Bacterial Culture - 29-8-23






CBP - 29-8-23











Comments
Post a Comment